Workers Comp Mileage Reimbursement Form
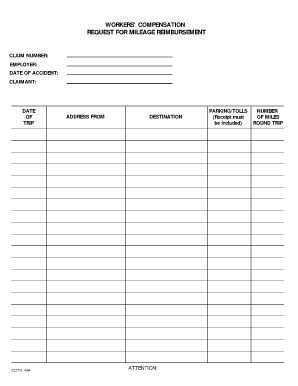
Do not send the original or a copy to the local Workers. Submit the completed form and copies of all receipts or bills to the workers compensation insurance carrier or to your employer if self-insured and to the Workers Compensation Board.
 28 Printable Mileage Reimbursement Request Form Templates Fillable Samples In Pdf Word To Download Pdffiller
28 Printable Mileage Reimbursement Request Form Templates Fillable Samples In Pdf Word To Download Pdffiller
Medical Travel Refund Request.

Workers comp mileage reimbursement form. All the forms you need when dealing with workers compensation and the Department of Industrial Accidents DIA. 44 rows Vocational rehabilitation invoice form. Form 114 KENTUCKY DEPARTMENT OF WORKERS CLAIMS Frankfort Kentucky 40601 REQUEST FOR PAYMENT FOR SERVICES OR REIMBURSEMENT FOR COMPENSABLE EXPENSES TO BE FILED WITH THE RESPONSIBLE EMPLOYER OR ITS PAYMENT OBLIGOR â Name address and Workers Compensation claim number of Employee for whom services were provided or expenses.
47 rows Form 16. The DIA uses forms for many reasons. It is extremely important that you document your travel accurately and submit mileage forms and supporting documentation to your attorney regularly.
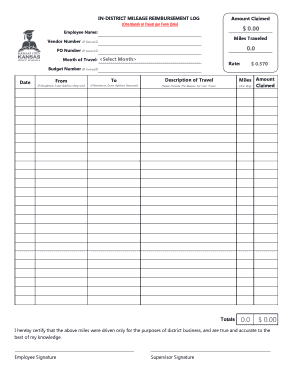
TransportationTravel Expenses Process Instructions Mileage Reimbursement Rate Updates to the mileage reimbursement rate can be viewed on the Commissions website at. Mileage rate is 56 cents 056 per mile. Total miles X state mileage rate amount reimbursed.
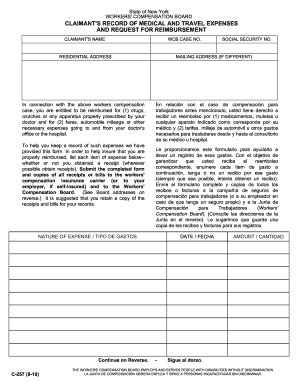
The lists are broken down into numbered and alphabetical lists. En relación con el caso de compensación para. Agreement for Permanent DisabilityDisfigurement Compensation.
This form is completed by the agency in conjunction with the injured employee to designate hisher election to utilize or not utilize accrued leave during the interim period andor to supplement lost wage workers compensation benefits on an approved workers compensation claim. Date Location Meals HotelLodging. This employee mileage reimbursement form presents the employee information like name campus-wide ID campus extension unit details fund department program class product and project.
20 CFR 725406 and 725701 and the Energy Employees Occupational Illness Compensation Program Act of 2000 42 USC 7384 and. This form is used by the insurer to voluntarily admit responsibility for payment of workers compensation benefits where a fatality has occurred. The Department of Workers Claims is the agency primarily charged with the administration of the Kentucky program and has exclusive jurisdiction over workers compensation claims.
Requesting travel reimbursement benefits To request this benefit complete the C-60 Injured Worker Reimbursement Rates for Travel Expense form and C-60A Completing the Injured Worker Statement for Reimbursement of Travel Expense form. Medical mileage expense form - EnglishSpanish. Workers Compensation Board Online Services Download Claim Notices eCase eClaims Administrators eClaims Data Entry eClaims Inquiry IC Inquiry Medical Portal Medical Portal Administrators Payer Compliance Proof of Coverage-DBPFL Proof of Coverage-WC Submit Claim Forms Submit Medical Forms Virtual Hearings XML Forms Submission.
In summary mileage reimbursement is an important benefit of filing a workers compensation claim and can provide some relief from the financial burden of a work-related injury. Medical mileage expense form. Not all forms have a number so if you cant find the form youre looking for check.
The Form 30D includes a map of Connecticuts 169. Httpsfmxcpastatetxusfmtraveltravelratesphp for the state mileage rate or call us at 800 252-7031. Send the original to the insurance company and keep a copy.
Our website is designed to provide users with helpful information on the functions of the Commonwealths workers compensation program. Send receipts for these costs. DAS Form WC-715 - Request for Use of Accrued Leave With Workers Compensation.
Mileage for reasonable travel to the pharmacy parking bridge tolls public transportation and other travel-related costs are also included. The Form 30D DEPENDENTS NOTICE OF CLAIM TO COMMISSIONER AND TO EMPLOYER is to be completed and filed by a dependent or dependents attorneyrepresentative for making a claim for workers compensation death benefits pursuant to Section 31-306 of the Workers Compensation Act. Overnight stays and meals.
For more information about workers. If you need a medical mileage expense form for a year not listed here please contact the Information and Assistance Unit at your closest district office of the Workers Compensation Appeals Board. This report is authorized by the Federal Employees Compensation Act 5 USC 8103a the Black Lung Benefits Act 30 USC 901.
The details of traveling like date and purpose of travel start and end city names miles traveled and reimbursement mileage are mentioned. Employer reimbursement is not subject to the minimum mileage requirements that apply to BWCs travel reimbursement. Office of Workers Compensation Programs.
For questions or assistance with completing this form please contact the Virginia Workers Compensation Commission toll-free at 1-877-664-2566. See Board address on reverse It is suggested that you retain a copy of the receipts and bills for your records. For travel on or after 1121.
It is an important legal document that provides an initial statement of the amount of benefits to be paid in a workers compensation case.
 Workers Compensation Mileage Reimbursement Form Fill Out And Sign Printable Pdf Template Signnow
Workers Compensation Mileage Reimbursement Form Fill Out And Sign Printable Pdf Template Signnow
 Final Invoice Legal Forms Form Legal
Final Invoice Legal Forms Form Legal
 Wc 10 Workers Comp Mileage Reimbursement Request Form Email Pdffiller
Wc 10 Workers Comp Mileage Reimbursement Request Form Email Pdffiller
 La Luba Workers Compensation Mileage Claim Form Fill And Sign Printable Template Online Us Legal Forms
La Luba Workers Compensation Mileage Claim Form Fill And Sign Printable Template Online Us Legal Forms
 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
 Ca Medical Mileage Expense Forms Workers Comp Mileage Reimbursement
Ca Medical Mileage Expense Forms Workers Comp Mileage Reimbursement
 26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 Job Description Template Free Job Description Template Fast Simple Copy Paste By Www Betterteam Com By Job Description Job Description Template Job
Job Description Template Free Job Description Template Fast Simple Copy Paste By Www Betterteam Com By Job Description Job Description Template Job
 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
 Final Report Of Guardian Of The Property Guardianship Probate Financial Information
Final Report Of Guardian Of The Property Guardianship Probate Financial Information
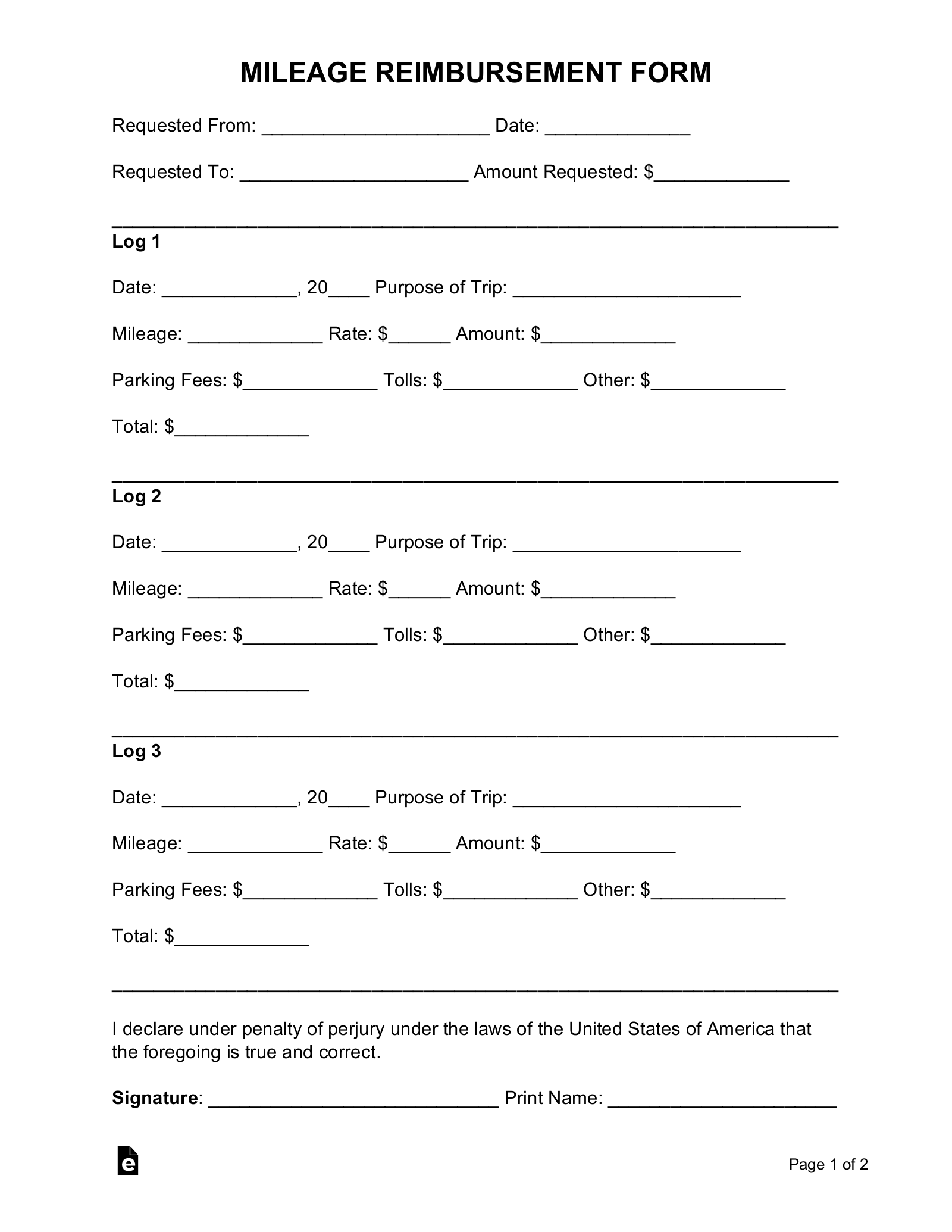 Free Mileage Reimbursement Form 2021 Irs Rates Word Pdf Eforms
Free Mileage Reimbursement Form 2021 Irs Rates Word Pdf Eforms
 Application For Retirement Of Mobile Home Certificate Of Title Real Property Ms Word
Application For Retirement Of Mobile Home Certificate Of Title Real Property Ms Word
 Excellent Work Excellent Work Flyer Digital Community Outreach Outreach Mileage
Excellent Work Excellent Work Flyer Digital Community Outreach Outreach Mileage
 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
 Free 11 Sample Mileage Reimbursement Forms In Ms Word Pdf Excel
Free 11 Sample Mileage Reimbursement Forms In Ms Word Pdf Excel
 Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 Mileage Reimbursement Form Workers Comp Page 3 Line 17qq Com
Mileage Reimbursement Form Workers Comp Page 3 Line 17qq Com
 26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
{kind=link}
Post a Comment for "Workers Comp Mileage Reimbursement Form"