Workers Comp Travel Reimbursement Form
Examples of medical documentation include but are. The forms are also available in individual listings.
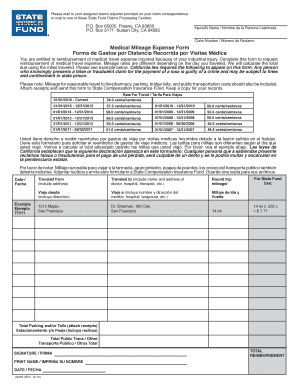 26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
208 rows Upon renewal of a workers compensation insurance policy a carrier may issue this.

Workers comp travel reimbursement form. Electronic sets of form numbers are limited to one thousand. BWC must authorize lodging in advance. Travel reimbursement is for reasonable travel expenses you incur attending medical and hospital services required as a result of an accepted work-related injury or illness.
Requesting travel reimbursement benefits. Physicians signature or facsimile is. This is a complete listing of all Division of Workers Compensation Forms.
OWCP Form 957-Medical Travel Refund Request. If the claim administrator disputes reimbursement a Claim Form can be filed with the Commission. O The last day of travel is 75 percent of the per diem rate 4125.
Florida Workers Compensation Uniform Medical TreatmentStatus Report Form Effective June 25 2006 Rev. Medical mileage expense form. Form 114 KENTUCKY DEPARTMENT OF WORKERS CLAIMS Frankfort Kentucky 40601 REQUEST FOR PAYMENT FOR SERVICES OR REIMBURSEMENT FOR COMPENSABLE EXPENSES TO BE FILED WITH THE RESPONSIBLE EMPLOYER OR ITS PAYMENT OBLIGOR â Name address and Workers Compensation claim number of Employee for whom services were provided or expenses.
Home d. See reverse side of form for complete instructions and attachment of receipts. For verification of each service date and type.
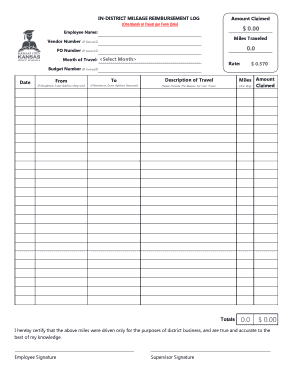
Employees are entitled to reimbursement of 056 per mile for travel for medical treatment provided they travel 20 miles or more roundtrip starting January 1 2021. Plan TimeCostTravel Encumbrance F245-454-000 Schedule of Future Payments for the Balance of the Permanent Partial Disability Award F207-162-000 Self-Insurer Accident Report SIF-2 Order Form paper SIF-2 form orders are limited to quantities of less than 400 until further notice. OWCP pays the claimant for travel to and from the medical provider to and from any therapy treatments and to and from the pharmacy for medicine used for the injuries.
The Form 30D includes a map of Connecticuts 169 cities and towns and their respective workers compensation districts as well as instructions for completing and filing this form. When requesting reimbursement for transportationtravel expenses the request must include a completed Claim Form TransportationTravel Expense Form receipts for travel expenses and medical documentation to support the expenses incurred. 1312008 -To access the interactive form right click the link.
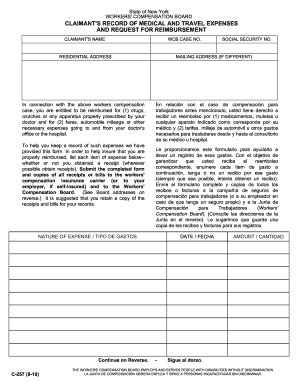
It includes reasonable costs associated with. If your travel reasonably includes an overnight stay you can get reimbursed for the cost of a hotel or other. In order to help insure that you are properly reimbursed list each item of expense below--whether or not you obtained a receipt wherever possible obtain receipts.
See Electronic Filing XML Format for more information about files with multiple submissions. No reimbursement is allowed for trips to purchase medications or supplies unless medically necessary. If you need a medical mileage expense form for a year not listed here please contact the Information and Assistance Unit at your closest district office of the Workers Compensation Appeals Board.
The Form 30D DEPENDENTS NOTICE OF CLAIM TO COMMISSIONER AND TO EMPLOYER is to be completed and filed by a dependent or dependents attorneyrepresentative for making a claim for workers compensation death benefits pursuant to Section 31-306 of the Workers Compensation Act. Submit the completed form and copies of all receipts or bills to the workers compensation insurance carrier or to your. Employees Claim Form PDF 114 kb Early Notification of Injury Form PDF 45 kb Direct Credit Application Form PDF 90 kb Information for Workers Rights Responsibilities PDF 78 kb Internal Dispute Resolution Process PDF 162 kb Medical andor Other Expenses Form PDF 76 kb Travel Reimbursement Form PDF 90 kb.
If you are seeking transportationtravel reimbursement please complete the TransportationTravel Expense Form and file directly with the claim administrator. Use this form to request reimbursement for claim-related medical or travel expenses. To request this benefit complete the C-60 Injured Worker Reimbursement Rates for Travel Expense form and C-60A Completing the Injured Worker Statement for Reimbursement of Travel Expense form.
Select save target as to save the form in your personal files. In some cases taxi travel. To get those rates go to httpsfmxcpastatetxusfmtraveltravelratesphp or call us at 800 252-7031.
Private motor vehicle including road tolls and car parking. Lodging Receipts are required. The amount reimbursed will be based on the travel rate for state employees.
If the claim administrator disputes reimbursement you may complete a Claim Form attaching the completed TransportationTravel Expense Form receipts and medical documentation to. O Full days of travel are 100 percent of the per diem rate 55. O The day of departure is 75 percent of the per diem rate 4125.
Employer reimbursement is not subject to the minimum mileage requirements that apply to BWCs travel reimbursement. Caution you must submit your request for travel pay on form OWCP Form 957 Medical Travel Refund Request within one year of the travel. Forms available for electronic filing are indicated by See Electronic Filing - Online Forms for more information about filing your PDF form online.
REQUIRED by BLACK LUNG. A traumatic injury is one that can be pinpointed to have occurred during one particular work shift falling down the steps for example. When the period of travel includes an overnight stay meal reimbursement is.
You need to complete either form CA-1 Federal Employees Notice of Traumatic Injury and Claim for Continuation of PayCompensation or form CA-2 Notice of Occupational Disease and Claim for Compensation. Special consideration will be given to employees who are totally disabled.
 Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
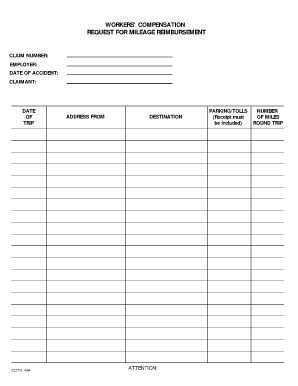 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
 129 Printable Mileage Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
129 Printable Mileage Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 La Luba Workers Compensation Mileage Claim Form Fill And Sign Printable Template Online Us Legal Forms
La Luba Workers Compensation Mileage Claim Form Fill And Sign Printable Template Online Us Legal Forms
 How Much Are Your Balls Worth A State By State Guide Workmans Comp Infographic Tomorrow News
How Much Are Your Balls Worth A State By State Guide Workmans Comp Infographic Tomorrow News
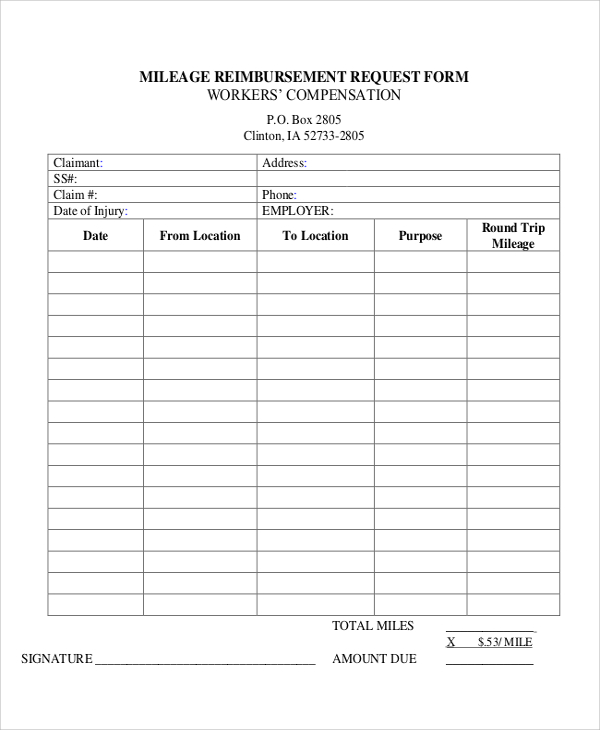 Free 11 Sample Mileage Reimbursement Forms In Ms Word Pdf Excel
Free 11 Sample Mileage Reimbursement Forms In Ms Word Pdf Excel
 Workers Compensation Mileage Reimbursement Form Fill Out And Sign Printable Pdf Template Signnow
Workers Compensation Mileage Reimbursement Form Fill Out And Sign Printable Pdf Template Signnow
Restaurant Employee Evaluation Form Best Of Free 7 Restaurant Employee Evaluation Forms In Pdf Evaluation Employee Employee Evaluation Form Evaluation Form
 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
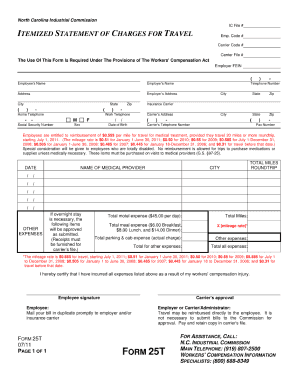 Form 25t Fill Online Printable Fillable Blank Pdffiller
Form 25t Fill Online Printable Fillable Blank Pdffiller
 Ca Medical Mileage Expense Forms Workers Comp Mileage Reimbursement
Ca Medical Mileage Expense Forms Workers Comp Mileage Reimbursement
 18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
18 Printable Workers Comp Mileage Reimbursement Forms And Templates Fillable Samples In Pdf Word To Download Pdffiller
 Job Description Template Free Job Description Template Fast Simple Copy Paste By Www Betterteam Com By Job Description Job Description Template Job
Job Description Template Free Job Description Template Fast Simple Copy Paste By Www Betterteam Com By Job Description Job Description Template Job
 Wc 10 Workers Comp Mileage Reimbursement Request Form Email Pdffiller
Wc 10 Workers Comp Mileage Reimbursement Request Form Email Pdffiller
 Final Report Of Guardian Of The Property Guardianship Probate Financial Information
Final Report Of Guardian Of The Property Guardianship Probate Financial Information
 28 Printable Mileage Reimbursement Request Form Templates Fillable Samples In Pdf Word To Download Pdffiller
28 Printable Mileage Reimbursement Request Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
26 Printable Medical Mileage Expense Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
Workers Comp Mileage Reimbursement Form Fill Online Printable Fillable Blank Pdffiller
 Forms Workflow Alncorp Google Search Outlook Calendar Calendar Make It Simple
Forms Workflow Alncorp Google Search Outlook Calendar Calendar Make It Simple
{kind=link}
Post a Comment for "Workers Comp Travel Reimbursement Form"